Table of Contents
Follow the general principles of orthopedic examination listed in the article below.
Exposure
Undress leaving the undergarments
Surface markings:
1. 1st palpable spinous process – C2
2. Hyoid – C3
3. Thyroid cartilage – C4/5
4. Cricoid cartilage – C6
5. Carotid tubercles (Chassaignac tubercle) – C6
6. Most prominent spinous process – C7
7. Longest spinous process – T1
8. Sternal notch – T3/4
9. Spine of scapula – T3
10. Inferior angle of scapula – T7
11. Highest point of iliac crest (Tuffier’s line) – L4/L5 interspace
12. Posterior superior iliac spine (PSIS) – S2
Standing position
Inspection
a. Ask to stand in Neutral Upright Spinal Alignment (NUSA) position: Standing with the knees and hips comfortably extended, the shoulders and neck neutral
Mnemonic: SADS
- Skin:
- Lumps or bumps (swellings)
- Erythema
- Ecchymosis
- Sinus
- Scars
- Hairline
- Abnormal tuft of hair (faun tail = flame shaped hairy patch)
- Dimple
- simple = <0.5 cm diameter and <2.5 cm from anal verge
- atypical = >0.5 cm diameter and >2.5 cm from anal verge
- Cafe-au-lait spots
- coast of California (neurofibromatosis): C = smooth = smooth border
- coast of Maine (McCune Albright): M = ragged = ragged border
- Atrophy: of visible muscles
- Deformity: Drop an imaginary plumb line and assess the alignment –
- Sagittal (lateral):
- Head – Through the ear lobes
- Shoulders – Through the acromion
- Thorax – Bisects the chest antero-posteriorly
- Lumbar area- Midway between the lumbar spine and abdomen and slightly anterior to the sacroiliac joint
- Hips – Posterior to the hip, through the greater trochanter
- Knee – Slightly anterior to the center of knee
- Ankle – Just in front of lateral malleolus through the tuberosity of 5th metatarsal
- Coronal (posterior):
- Head – Bisects the head through the external occipital protuberance
- Shoulders – Midway between the shoulders
- Trunk – Bisects the trunk
- Pelvis – Through the gluteal cleft
- Knee – Equidistant from both knees
- Ankle- Equidistant from both malleoli
- Sagittal (lateral):
- Symmetry:
- Anterior:
- Head: Eyes, Ears and Head tilt
- Neck: Sternocleidomastoid prominence
- Shoulders
- Nipples and shape of thorax
- ASIS
- Knees and patellae
- Forefoot
- Posterior:
- Head position
- Level of shoulder
- Level of scapula and distance from spine
- Central furrow of spine and paraspinal muscle prominence
- Thorax (ribs)
- Iliac crest and PSIS (dimple of Venus)
- Gluteal crease
- Popliteal crease
- Heels
- Anterior:
b. Ask to bend forwards (Adam’s forward bend):
- Look for rib prominence (structural scoliosis) after ruling out limb length discrepancy
c. Ask to bend sidewards if scoliosis:
- To assess flexibility of curve
Palpation
a. Local temperature
b. Pinch skin folds: Widespread superficial tenderness may indicate functional overlay (Wadell’s sign)
c. Paraspinal muscles:
- Spasm: Ask to bend towards the affected side (doesn’t soften and relax but remains firm in spasm)
- Trigger points
d. Spinous process: Localize pathology using anatomical landmarks
- Tenderness:
- Direct: over spinous process
- Rotatory: twist side of spinous process
- Thrust: gentle thumping
- Step off: Spondylolisthesis (palpable usually from Meyerding’s Grade III)
e. Transverse processes
f. Facet joints: Between spinous process and transverse processes (~2-3 cm from spinous process)
g. Iliac crests and PSIS
Range of Motion (ROM)
Look for quantity and quality (smoothness and pain) –
| Movements | Range of motion (ROM) | Goniometer – stationary and moving arms | Other methods of assessment |
| Flexion | 45-60 degrees | Mid-axillary line at the level of lowest rib | a. Finger tip to floor distance (depends on hamstring flexibility): normally 7 cm or less b. Position of fingers reaching leg (eg. tibia shin, knee, etc.) c. Schober’s test (lumbar spine): increase in distance between 2 points (midpoint of line joining 2 PSIS and a point 10 cm above it) >5 cm d. Modified Schober’s test (lumbar spine): increase in distance between 2 points (5 cm below PSIS midpoint and 10 cm above PSIS midpoint) >5 cm e. Ott’s test (thoracic spine): increase in distance between 2 points (C7 spinous process and a point 12 inches/30 cm distal to it) >3 cm f. T1-L1 distance >8 cm and L1-S1 distance >8 cm |
| Extension | ~30 degrees | As above | Distance decreased between L1 and S1 can also be measured |
| Lateral bending | ~30 degrees | C1 to S1 spinous process | a. Finger tip to floor distance: normally <10 cm b. Increase in distance between 2 points (level of dimple of venus at mid-axillary line and a point 10 cm above) > 3 cm c. Position of fingertips reaching leg |
| Rotation (hips anchored by examiner or in sitting position with arms folded on chest) | ~40 degrees | Center = Center of head Stationary arm = Line joining 2 ASIS Moving arm = Line joining 2 acromion process | Increase in distance between ipsilateral acromion tip and contralateral greater trochanter of femur Waddel’s distraction testing: Note the amount of rotation required to produce pain in the back. Now ask the patient to keep his hands firmly at his sides and repeat: the major part of the movement will take place in the legs and the pain occurring with the same amount of apparent rotation suggests functional overlay |
Limitations and pain in:
- Flexion: Pain protection, Ankylosing spondylitis, Normal elderly
- Extension: Facet joint arthrosis, Spondylolisthesis, Spondylolysis, Spinal canal stenosis
- Lateral flexion: Herniated discs on same side
Measurements
1. Head tilt: Interpupillary angle
2. Shoulder tilt: Intercoracoid angle
3. Trunk inclination: Angle of plane of greatest rib or lumbar hump in forward bent position
4. Chin-brow vertical angle: Angle between line connecting chin-forehead with vertical line
5. Pelvic obliquity: Intercrest or Inter-ASIS angle
6. Lumbar lordosis: Keep tape measure tensed between thoracic and spinal prominences and measure the distance of concavity of lumbar spine from it (normally >2 cm)
7. Sciatic list: Drop a plumb line from lower thoracic convexity and measure the offset from gluteal cleft
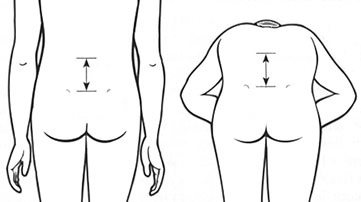
8. Rib-pelvis distance: Distance between inferior margin of ribs and superior edge of iliac crest in mid-axillary line in finger-breadths (</= 2 is considered positive for kyphosis due to occult lumbar vertebral fractures)
9. Wall-occiput distance: Distance between wall and occiput when patient is asked to stand on wall touching the occiput and heels to the wall (>0 is considered positive for kyphosis due to occult thoracic vertebral fractures)
10. Chest expansion: at rest and peak of inspiration measured at nipple line (<2.5 cm is considered positive)
Screen tests
1. Romberg test (Dorsal column)
2. Squat and get up (L3)
3. Walk on heels (L4)
4. Stand on one leg/Trendelenburg test (L5)
5. Walk on tip toes (S1)
Gait
Provocative tests
1. Quadrant test or Kemp’s test: Assist the patient in extending the spine maximally holding the shoulders, then ask patient to rotate and lateral flex to the site of pain –
- Symptoms more concordant to those of neurogenic claudication: Lumbar spinal stenosis
- Pain predominant: Facet joint arthrosis
2. Stork test: Extension of spine standing on one leg, then clinician passively hyper-extends and rotates the patient towards weight bearing side
- Pain reproduction: Spondylolysis and possible spondylolisthesis
Sitting position
Obliteration of abnormal curvatures of spine visible on standing suggests the curve is compensatory (may be secondary to limb length discrepancy)
Provocative test
1. Bechtrew’s test (seated SLR): can be undertaken as a part of flip test (Waddel’s sign)
2. Slump test: ask the patient to flex spine (slump), followed by passive neck flexion, active knee extension and dorsiflexion of foot (positive nerve root tension sign if pain) and relieved on returning neck to neutral
3. Tripod sign: passively extend the patient’s knee (patient will lean backwards with support of hands or slump forwards in hamstring contractures)
4. Naffziger’s test: Jugular compression leading to pain in lumbar region suggests intrathecal space occupying lesion in lumbar region (can also use Valsalva maneuver)
Supine position
Neurological examination
1. Higher functions (assess at time of history taking): consciousness, alertness, orientation, speech
2. Motor:
- Bulk
- Tone (modified Ashworth scale for grading)
- Power
- Co-ordination (heel-shin test, finger nose test)
- Involuntary movements
3. Reflex:
- Superficial
- Abdominal (T7-12)
- Cremasteric (L1-2)
- Plantar response (L5,S1)
- Deep
- Knee jerk (L3,L4)
- Medial hamstring (L5)
- Ankle (S1)
- Clonus (patellar, ankle): Sustained = >5 beats
4. Sensory:
- Superficial:
- Pain (pin prick)
- Fine touch (wisp of cotton)
- Temperature (test tubes containing hot and cold water or tuning fork)
- Deep:
- Joint position sense
- Vibration sense (128 Hz tuning fork)
- Cortical:
- 2 point discrimination
- Stereognosis
| NERVE ROOT | MOTOR | SENSORY | REFLEX |
|---|---|---|---|
| L2 | Iliopsoas (Resisted hip flexion) | Mid-anterior thigh | None |
| L3 | Quadriceps (Resisted knee extension) | Medial femoral condyle | Patellar |
| L4 | Tibialis anterior (Resisted ankle dorsiflexion and inversion) | Medial malleolus | Patellar |
| L5 | Extensor hallucis longus an Extensor digitorum longus (Resisted great-toe dorsiflexion); Resisted ankle eversion; Gluteus medius (abduction) | 1st web space | Hamstring or Semitendinosus reflex |
| S1 | Tendo-achilles, Flexor hallucis longus, Flexor digitorum longus (Resisted ankle plantar flexion) | Lateral plantar foot | Achilles |
5. Sudomotor examination:
- Stroke the skin with finger or barrel of pen: pulls smoothly over dry (symathectomized) skin but irregularly and unevenly over normal moist skin
- Starch-iodine test (Minor’s test):
- Tincture-iodine is applied to skin and allowed to air-dry
- Dried area is dusted with cornstarch or potato flour
- Sweating is encouraged by increasing room temperature, exercise or pilocarpine
- Sweat causes starch and iodine to combine and change to dark blue color
Provocative tests
1. Straight leg raising test (SLRT) or Lasegue’s test and sensitizers (Braggard, Soto-hall, Bow string tests):
2. Well’s crossed leg SLRT (Fajersztajn test): more specific; may indicate large paracentral disc herniation
3. Hoover’s test (for functional weakness): The patient is unable to extend the hip and to press the heel into the bed on request. The hip is extended involuntarily when the opposite leg is lifted off the bed.
4. Tests for SI joints and hips
Prone position
Femoral nerve stretch test (for L3-L4): Flex the patient’s knee and lifting the hip into extension – pain may be elicited down the front of the thigh
Lateral position
1. Sciatic point palpation
2. Saddle area sensation (S3, S4)
3. Per rectal:
- Anal reflex (S3, S4)
- Bulbocavernosus reflex (S3, S4)