While we have more sophisticated radiological techniques of examination of the mastoids, the ability to read an X-ray of mastoid is a must for the undergraduate students of the medicine. While describing an X-ray in ENT or Otorhinolaryngology, you need to comment on these points:
- Plain or Contrast
- Regions: Mastoid, Nose and PNS or Soft-tissue neck
- View: AP, lateral, other views of mastoid x-rays
- Important anatomical landmarks
- Pathological findings
- Diagnosis
And when reading an X-ray of mastoid, never forget to comment on the following points:
- Type of pneumatization: cellular (well pneumatized), acellular (sclerotic), diploetic
- Position of: dural plate, sinus plate
- Presence of bone destruction
- Presence of mastoid cavity
- Presenc of choleasteatoma
The adult temporal bone is made up of squamous, mastoid, petrous and tympanic parts. The standard projections for the radiographic examination of mastoid include:
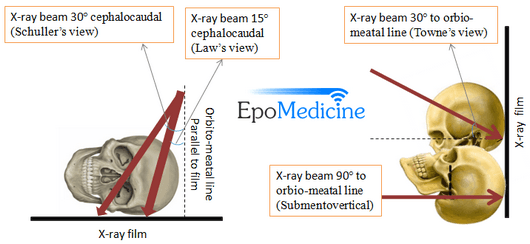
- Law’s view (15º lateral oblique): Sagittal plane of the skull is parallel to the film and X-ray beam is projected 15 degrees cephalocaudal
- Schuller’s or Rugnstrom view (30º lateral oblique): Similar to Law’s view but cephalocaudal beam makes an angle of 30 degrees instead of 15 degrees
- Stenver’s view (Axio-anterior oblique posterior): Facing the film and head slightly flexed and rotated to 45 degrees to the opposite of side under examination and X-ray beam is angulated 14 degrees caudad
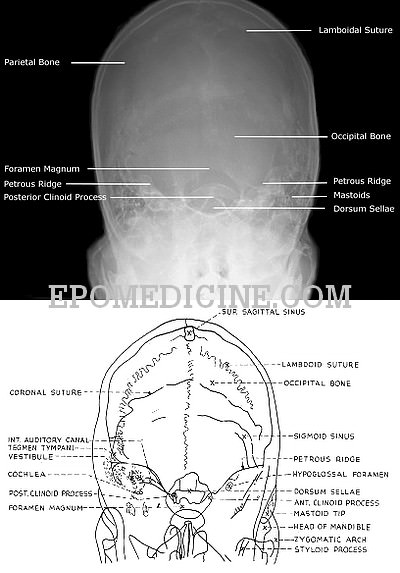
- Towne’s view (30º Fronto-occipital axial): Anteroposterior view with 30 degrees tilt from above and in front
- Transorbital view (Anteroposterior or Posteroanterior): AP or PA view with orbito-meatal line perpendicular to the film and the X-ray beam also perpendicular to the film.
- Submentovertical view (Full axial): Chin raised and neck hyperextended until orbito-meatal line is parallel to the film and the beam is projected at right angles to the film from submental area
- Other views: Mayer’s view, Owen’s view, Chause III view

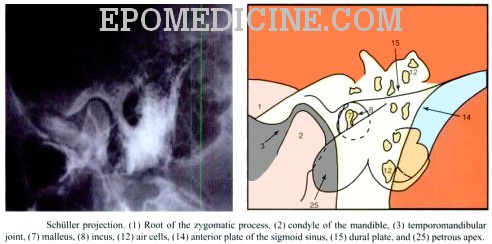
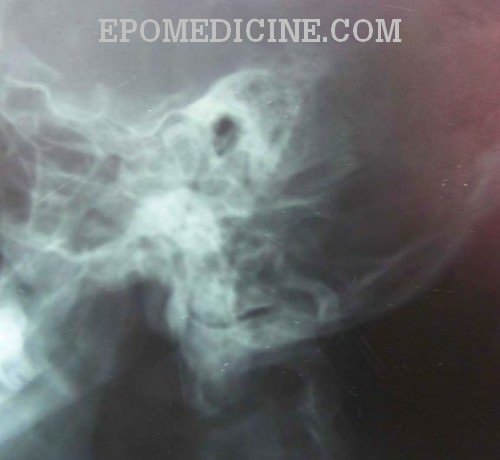
Notes on Schuller’s view:
In schuller’s view, there is superimposition of External Acoustic Meatus (EAC) and Internal Acoustic Meatus (IAM) due to the angulation of the X-ray beam. This angulation is provided to separate the right and left mastoid. This angulation also displaces the arcuate eminence of the petrous bone downward showing the key area i.e. antrum and upper part of attic area which is not clearly seen in the Law’s view. This is how, Schuller’s view differs from the Law’s view.
| X-ray projection | Structures seen | Clinical applications |
| Schuller’s view | EAC superimposed on IAC Mastoid air cells Tegmen Lateral sinus plate Condyle of mandible Sino-dural angle Attico-antral region (Key area) | Extent of pneumatization (compare both sides) Destruction of intercellular septa (mastoiditis) Location of sinus plate (position of sigmoid sinus) & tegmen Cholesteatoma Longitudinal fracture of petrous pyramid |
| Towne’s view | Both side temporal bone Arcuate eminence Superior semicircular canal Mastoid antrum IAC, tympanic cavity, cochlea EAC | Acoustic neuroma Apical petrositis |
Some radiological signs in mastoid conditions:
1. Normal: Cellular (80%)/Bilaterally acellular (20%) – If cellular, mastoid cells are seen extending beyond sinus plate and tegmen
2. Acute mastoiditis: Diffuse haziness or clouding of mastoid air cells, destruction of intercellular septa (loss of trabecular pattern) and the lateral sinus plate appears more prominent
3. Chronic mastoiditis: Diffuse sclerosis of cellular mastoid and prominence of periantral triangle
4. Cholesteatomas: Cholesteatomas are radiolucent and can only be diagnosed if they erode bone. An erosion of mastoid antrum is seen as an area of translucency in a sclerotic mastoid.

Notes on Citelli’s or Sinodural angle:
Citelli’s angle or sinodural angle is the angle between the sinus plate and the dural plate. This angle is acute in primary sclerosis but obtuse in secondary sclerosis i.e. Chronic Suppurative Otitis Media (CSOM).
Differential diagnoses of Mastoid cavity:

- Choleasteatoma: cavity has smooth margins and is surrounded by a rim of sclerosis
- Granulation cavity: cavity shows hairline appearance
- Operated cavity: history of mastoid surgery, cavity shows irregular margin (due to osteogenesis) and sclerosis is absent
- Metastases
- Multiple myeloma
- TB mastoiditis
- Eosinophilic granuloma
- Large antral cells


it was good explanation…but lot more to do in this.
Its very informative and concise
thanks , good information,please update and expand it if possible
It is very good. But it would have been better if it was explained on x-ray plate.