For the purpose of remembering the clinical manifestations of upper motor neuron lesion (UMNL) and lower motor neuron lesion (LMNL), a mnemonic has already been devised and discussed here.
Now, it’s time to understand the anatomical and physiological basis of these manifestations.
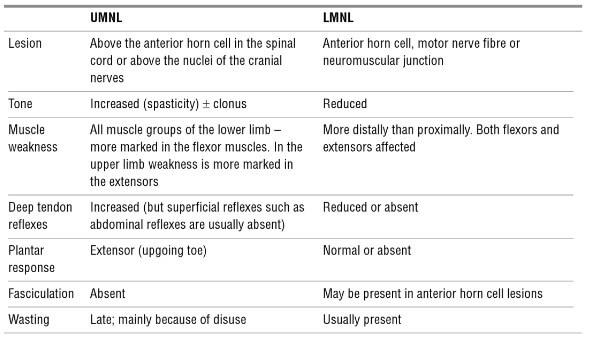
Upper Motor Neuron Lesion (UMNL) Syndrome
Acute Manifestations
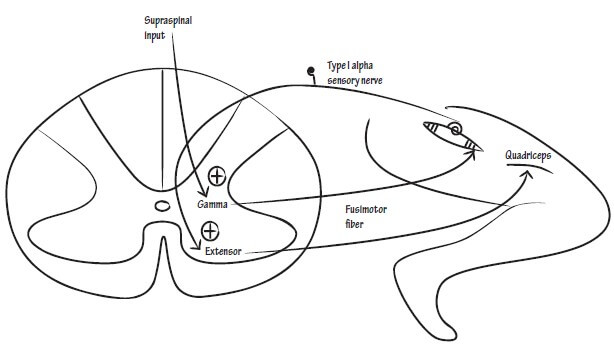
1. Spinal shock: Hypotonia and loss of all reflexes on contra-lateral side
- Gamma-motor neurons by stretching muscle spindle bodies, activate alpha-motor neurons leading to extrafusal muscle contraction.
- In upper motor neuron lesion, supraspinal excitatory input to gamma-neurons is lost.
2. Relative sparing of trunk muscles:
- Trunk muscles are bilaterally innervated by anterior corticospinal tract, so that a lesion of one side of the tract has minimal/imperceptible manifestations.
- Distal muscles, fingers, toes, fine articulations and flexors more than extensors are handled by lateral corticospinal tract and affected more.
Late Manifestations
1. Babinski sign:
- It is a primitive response present normally in newborns.
- The extensor response is modified to flexor response by developing corticospinal tract.
- Upper motor neuron lesion results in reappearance of primitive extensor response.
2. Spasticity:
- Spasticity is increased muscle tone, hyperactive stretch reflexes and clonus.
- Due to removal of inhibitory influences exerted by cortex on postural centers of vestibular nuclei and reticular formation.
- The mechanism has already been discussed in detail in Clonus.
3. Hyporeflexia of superficial reflexes:
- Superficial reflexes are absent in infants and appear after about 6 months to 1 year.
- Their appearance may depend upon the myelination of the corticospinal tract.
- Hence, in upper motor neuron lesion, superficial reflexes may be lost.
- It may even be absent in normal individuals, hence, correlation with other corticospinal signs is necessary. 1
4. Contralateral or Ipsilateral Involvement:
- Pyramidal decussation occurs at the level of medulla-spinal cord junction.
- Lesion above pyramidal decussation leads to contralateral signs.
- Lesion below pyramidal decussation leads to ipsilateral signs.
5. Involvement below the lesion:
- Damage of UMN below the level of lesion.
6. Decorticate posture:
- Occurs in UMNL above the red nucleus – hence, rubrospinal tract still working.
- This leads to release of cortical inhibition of the rubro-, reticulo-, and vestibulospinal tracts. In this circumstance, the action of rubrospinal tract supercedes that of the reticulo- and vestibulospinal tracts, which results in arm flexion at the elbows and lower extremity extension, so-called decorticate posturing.
Rubro-spinal tract regulate flexor tone in upper limb.
Reticulo- and vestibulo-spinal tracts regulate extensor tone in the neck and both the upper and lower limbs.
7. Decerebrate posture:
- Occurs in UMNL below the red nucleus – hence, rubrospinal tract not working.
- This releases inhibition of the reticulo- and vestibulospinal tracts, which results in extension of the neck and all four limbs, so-called decerebrate posturing.