A. Osteology:
1. Femur:
- Largest bone in the body
- Distal femur possess 2 condyles of which the medial one is larger
- Medial epicondyle is more porminent and supports the adductor tubercle
2. Patella (Knee cap):
- Largest sesamoid bone
- Functions:
- fulcrum for quadriceps
- protects knee joint
- enhances lubrication and nutrition of knee
- Accessory or “bipartite” patella: may represent failure of fusion of the superolateral corner of the patella and is commonly confused with patellar fractures.
3. Tibia:
- 2nd largest bone in the body
- Intercondylar eminence:
- separates medial (oval and concave) condyle or facet and lateral (circular and convex) condyle or facet.
- separates anterior and posterior cruciate ligaments
- Tibial tubercle: elevation located on anterior surface of tibia where patellar tendon inserts.
- Gerdy’s tubercle: elevation located on lateral surface of proximal tibia where iliotibial tract inserts.
4. Fibula:
- Styloid process of head: attachment for fibular collateral ligament and biceps tendon
- Neck: grooved by common peroneal nerve
B. Arthrology:
- Knee joint is the largest joint in the body.
- Type of joint: Compound joint
- Tibio-femoral joint: Modified hinge or condyloid joint
- Patello-femoral joint: Sellar or saddle joint
- Articulation: Medial and lateral femoral condyles articulate with the corresponding tibial condyles or facets
C. Ligaments of Knee:
| Ligament | Origin | Insertion | Function |
| Ligamentum patellae | Patella | Tibial tuberosity | Stabilizes patellofemoral joint |
| Retinacular | Vastus medialis and lateralis | Tibial condyles | Forms anterior capsule |
| Posterior fibers | Femoral condyles | Tibial condyles | Forms posterior capsule |
| Oblique poplitieal | Semimebranosus tendon | Lateral femoral condyle/posterior capsule | Strengthens capsule |
| Deep Medial Collateral (MCL) | Medial epicondyle | Medial meniscus | Holds medial meniscus to femur |
| Superficial MCL | Medial epicondyle | Medial condyle of tibia | Resists valgus force |
| Arcuate | Lateral femoral condyle, over popliteus | Posteriot tibia/fibular head | Posterior support |
| Lateral collateral (LCL) | Lateral epicondyle | Lateral fibular head | Resists varus force |
| Anterior cruciate (ACL) | Anterior intercondylar tibia | Posteromedial lateral femoral condyle | Limits hyperextension/sliding |
| Posterior cruciate (PCL) | Posterior sulcus tibia | Anteromedial femoral condyle | Prevents hyperflexion/sliding |
| Coronary | Meniscus | Tibial periphery | Meniscal attachment |
| Wrisberg | Posterolateral meniscus | Medial femoral condyle (behind PCL) | Stabilizes lateral meniscus |
| Humphrey | Posterolateral meniscus | Medial femoral condyle (in front) | Stabilizes lateral meniscus |
| Transverse meniscal | Anterolateral meniscus | Anteromedial meniscus | Stabilizes menisci |
About Menisci or Semilunar cartilages:
Functions:
- Makes the articular surface more congruent (surface of joints are equal)
- Serve to deepen the concavity of tibial condyles
- Shock absorbers
- Lubricates the joint cavity
- Gives rise to proprioceptive impulses (sensory function due to nerve supply)
Blood supply:
- Peripheral 1/3 rd: vascular and can be repaired
- Inner 2/3 rd: nourished by synovial fluid
Shape:
- Medial meniscus: Larger with open “C” configuration (nearly semicircular)
- Lateral meniscus: Smaller with closed “C” configuration (nearly circular)
About Cruciate ligaments:
- Anterior cruciate ligament is composed of an anteromedial portion that is tight in flexion and a posterolateral portion that is tight in extension.
- Posterior cruciate ligament has an anterolateral portion that is tight in flexion and posteromedial portion that is tight in extension.
Note: All the ligaments of knee are extracapsular except cruciate ligaments and menisci which are instracapsular.
Locking and Unlocking of Knee:
1. Locking: Full extension → Taut anterior cruciate → No further symmetrical extension → Medial femoral condyle moves back – lateral condyle moves forward → Femur internally rotates on tibia on axis of anterior cruciate ligament → Medial/lateral collateral and oblique popliteal ligaments tighten → Tensor fascia lata and gluteus maximus tighten iliotibial tract → Knee hyperextends and locks
Summary: Locking occurs as a result of internal rotation of femur during last stage of extension and is produced by quadriceps femoris. It allows knee to remain in the position of full extension as in standing without much muscular effort.
2. Unlocking: Popliteus externally rotates femur on tibia → Locked ligaments loosen → Hamstrings can then flex knee
Summary: It is the reversal of locking brought by popliteus muscle.
D. Muscles of the Knee:
| Location | Muscles | Attachment at Knee | Action at Knee |
| Anterior | Quadriceps femoris (Rectus femoris, Vastus- medialis, intermedius, lateralis) | Patella and patellar ligament | Knee extension |
| Lateral | Biceps femoris | Head of fibula and lateral condyle of tibia | Knee flexion and external rotation |
| Popliteus | Upper posteromedial surface of tibia | Knee flexion and internal rotation | |
| Medial | Pes anserinus (Sartorius, gracilis, semitendinosus) | Anteriomedial surface of proximal tibial, just below condyle | Knee flexion and internal rotation (semitendinosus); external roatation (Sartorius) |
| Semimembranosus | Posteromedial surface of medial tibial condyle | Knee flexion and internal rotation | |
| Posterior | Medial and lateral head of gastrocnemis | Posterior surface of femur, near or on respective condyles | Knee flexion |
| Plantaris | Lateral supracondylar ridge of femur above gastrocenmius | Knee flexion |
Note: Biceps femoris, semitendinosus and semimembranosus forms the Hamstring muscles which are the major flexors of the knee joint.
E. Bursae of Knee:
There are 13 bursae around knee – 4 Anterior, 2 Medial, 2 Lateral and 4 Posterior
F. Blood supply of Knee:
Genicular arteries:
- Popliteal gives: superior (medial and lateral), middle, inferior (medial and lateral)
- Femoral gives: descending branch from profunda
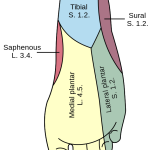
G. Nerve supply of Knee:
- Femoral nerve to vasti
- Sciatic nerve, through direct genicular branches
- Obturator nerve, through posterior division
H. Radiographic anatomy of Knee:
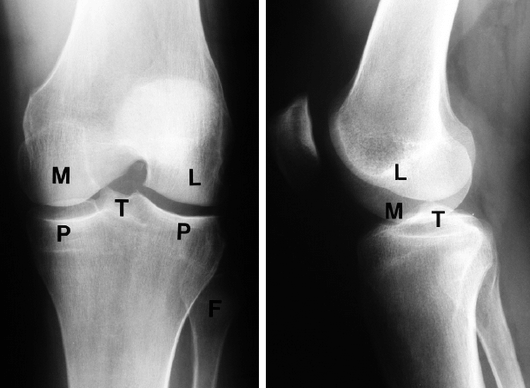
M – Medial femoral condyle
L – Lateral femoral condyle
T – Tubercles of intercondylar eminence
P – Medial and lateral tibial plateaus
F- Head of fibula
Anteroposterior (AP) and lateral views are essential in the diagnosis of knee disorders. A tunnel view visualizes the intercondylar notch, and tangential views are helpful in diagnosing patellar disorders. With patients over the age of 40, the anteroposterior view should always be performed with the patient standing. This may reveal subtle joint space narrowing if osteoarthritis is present.
 I. Normal Alignment of Knee:
I. Normal Alignment of Knee:
Slight valgus position: angle between longitudinal axis of femur and tibia is 170º opened laterally
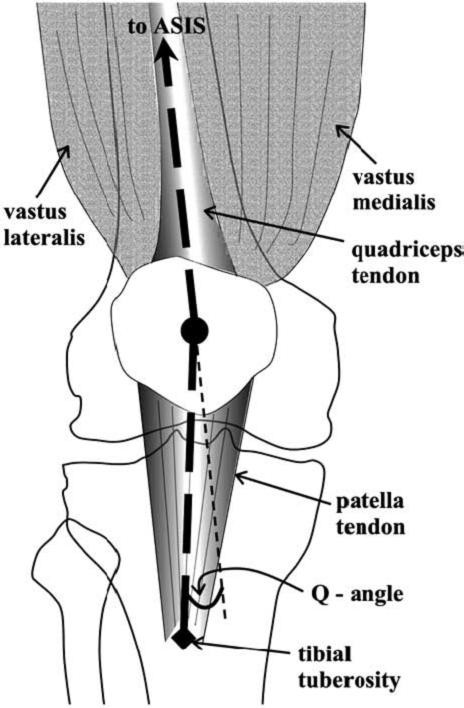
Q angle (Quadriceps angle): is a measure of the axis of pull of the quadriceps tendon and that of the ligament of the patella. The former is measured by a line drawn from the ASIS (Anterior superior iliac spine) to center of patella. The latter is determined by a line drawn from the tibial tuberosity to the center of the patella. The normal Q angle is between 15 -20º. This angle is somewhat greater in females than males. A Q angle much greater than normal means the patella will track in a lateral direction rubbing against the lateral femoral condyle causing Patella pain.
J. Functional anatomy of knee:
a. Flexion:
- Active: Upto 120º with hip extended and upto 140º with hip flexed
- Passive: Upto 160º
b. Extension: 0 to 10º above horizontal plane
J. Applied anatomy of Knee:
1. Degenerative diseases: Knee is the commonest site for osteoarthritis.
2. Infection: Knee is the commonest site for spetic arthritis.
3. Deformity/Malalignment:
- Genu valgum or Knock knee: Tibia abducted with respect to femur (> 170º)
- Genu varum or Bow leg: Tibia adducted with respect to femur (< 170º)
4. Ligamentous Injuries:
Anterior Cruciate Ligament (ACL) Stability Tests
- Lachman Test (most sensitive)
- Knee Anterior Drawer Test
- Pivot Shift Test (MacIntosh Test)
Posterior Cruciate Ligament (PCL) Tests
- Knee Posterior Drawer Test
- PCL Sulcus Test
- PCL Sag Test
Collateral ligament evaluation
- Knee Valgus Stress Test (Medial collateral ligament)
- Knee Varus Stress Test (Lateral collateral ligament)
Meniscus Evaluation
- McMurray’s Test
- Apley’s Compression Test and Apley’s Distraction Test
- Bounce Test
- Thessaly Test
- Inability to fully extend knee may suggest “bucket-handle” meniscal tear